
AMEE Guides in
Medical Education
www.amee.org
Program evaluation models and
related theories
Ann W Frye
Paul A Hemmer
AMEE GUIDE
67
Theories in Medical Education

Program evaluation models and related theories
Institution/Corresponding address:
Ann W Frye
Ofce of Educational Development
University of Texas Medical Branch
301 University Boulevard
Galveston, Texas 77555-0408
USA
Tel: +409-772-2791
Fax: +409-772-6339
Email: [email protected]
The authors:
Ann W Frye, PhD, is Director of the Ofce of Educational Development and Assistant Dean for Educational
Development at the University of Texas Medical Branch, Galveston, Texas. She specializes in educational
evaluation and research in the medical education context.
Paul A Hemmer, MD MPH, is Professor and Vice Chairman for Educational Programs, Department of Medicine,
Uniformed Services University of the Health Sciences, F. Edward Hebert School of Medicine, Bethesda, MD, USA.
This AMEE Guide was rst published in Medical Teacher:
Frye AW, Hemmer PA (2012). Program evaluation models and related theories. Medical Teacher, 34(5): e288-99.
Guide Series Editor: Trevor Gibbs ([email protected])
Production Editor: Morag Allan Campbell
Published by: Association for Medical Education in Europe (AMEE), Dundee, UK
Designed by: Cary Dick
© AMEE 2013
ISBN: 978-1-908438-18-8

Guide 67: Program evaluation models and related theories
Contents
Abstract .. .. .. .. .. .. .. 1
Introduction .. .. .. .. .. .. 2
A focus on change .. .. .. .. .. .. 2
Program evaluation dened .. .. .. .. .. 3
Reasons for program evaluation .. .. .. .. .. 3
Theories that inform educational program evaluation models .. .. 4
Reductionism .. .. .. .. .. .. 4
System theory .. .. .. .. .. .. 5
Complexity theory .. .. .. .. .. .. 6
Common evaluation models .. .. .. .. .. 8
The experimental / quasi-experimental models .. .. .. .. 8
Kirkpatrick’s four-level evaluation model .. .. .. .. .. 10
The Logic Model .. .. .. .. .. 12
The CIPP (Context / Input / Process / Product) model .. .. .. 15
Conclusion .. .. .. .. .. .. .. 20
References .. .. .. .. .. .. .. 21
Recommended readings .. .. .. .. .. 22

Guide 67: Program evaluation models and related theories

1
Guide 67: Program evaluation models and related theories
Abstract
This Guide reviews theories of science that have inuenced the development
of common educational evaluation models. Educators can be more condent
when choosing an appropriate evaluation model if they rst consider the
model’s theoretical basis against their program’s complexity and their own
evaluation needs. Reductionism, system theory, and (most recently) complexity
theory have inspired the development of models commonly applied in
evaluation studies today. This Guide describes experimental and quasi-
experimental models, Kirkpatrick’s four-level model, the Logic Model, and the
CIPP (Context/Input/Process/Product) model in the context of the theories
that inuenced their development and that limit or support their ability to
do what educators need. The goal of this Guide is for educators to become
more competent and condent in being able to design educational program
evaluations that support intentional program improvement while adequately
documenting or describing the changes and outcomes – intended and
unintended – associated with their programs.
TAKE HOME MESSAGES
• Educational programs are fundamentally about change; program evaluation
should be designed to determine whether change has occurred.
• Change can be intended or unintended; program evaluation should examine
for both.
• Program evaluation studies have been strongly inuenced by reductionist
theory, which attempts to isolate individual program components to determine
associations with outcomes.
• Educational programs are complex, with multiple interactions among participants
and the environment, such that system theory or complexity theory may be
better suited to informing program evaluation.
• The association between program elements and outcomes may be non-linear
– small changes in program elements may lead to large changes in outcomes,
and vice-versa.
• Always keep an open mind – if you believe you can predict the outcome of an
educational program, you may be limiting yourself to an incomplete view of
your program.
• Choose a program evaluation model that allows you to examine for change
in your program and one that embraces the complexity of the educational
process.
Educators can be more
condent when choosing
an appropriate evaluation
model if they rst consider
the model’s theoretical
basis against their program’s
complexity and their own
evaluation needs.
2
Guide 67: Program evaluation models and related theories
Introduction
Program evaluation is an essential responsibility for anyone overseeing a
medical education program. A ‘program’ may be as small as an individual
class session, a course, or a clerkship rotation in medical school or it may be as
large as the whole of an educational program. The ‘program’ might be situated
in a medical school, during postgraduate training, or throughout continuing
professional development. All such programs deserve a strong evaluation
plan. Several detailed and well written articles, guides, and textbooks about
educational program evaluation provide overviews and focus on the ‘how to’
of program evaluation (Woodward, 2002; Goldie, 2006; Musick, 2006; Durning et
al., 2007; Frechtling, 2007; Stufebeam & Shinkeld, 2007; Hawkins & Holmboe,
2008; Cook, 2010; Durning & Hemmer, 2010; Patton, 2011). Medical educators
should be familiar with these and have some of them available as resources.
This Guide will be most helpful for medical educators who wish to familiarize
themselves with the theoretical bases for common program evaluation
approaches so that they can make informed evaluation choices. Educators
engaged in program development or examining an existing educational
program will nd that understanding theoretical principles related to common
evaluation models will help them be more creative and effective evaluators.
Similar gains will apply when an education manager engages an external
evaluator or is helping to evaluate someone else’s program. Our hope is that
this Guide’s focus on several key educational evaluation models in the context
of their related theories will enrich all educators’ work.
A focus on change
We believe that educational programs are fundamentally about change. Most
persons participating in educational programs – including learners, teachers,
administrators, other health professionals, and a variety of internal and external
stakeholders – do so because they are interested in change. While a program’s
focus on change is perhaps most evident for learners, everyone else involved
with that program also participates in change. Therefore, effective program
evaluation should focus, at least in part, on change: Is change occurring? What
is the nature of the change? Is the change deemed ‘successful’? This focus
directs that program evaluation should look for both intended and unintended
changes associated with the program. An educational program itself is rarely
static, so an evaluation plan must be designed to feed information back
to guide the program’s continuing development. In that way, the program
evaluation becomes an integral part of the educational change process.
In the past, educational program evaluation practices often assumed a simple
linear (cause-effect) perspective when assessing program elements and
outcomes. More recent evaluation scholarship describes educational programs
as complex systems with nonlinear relationships between their elements and
program-related changes. Program evaluation practices now being advocated
account for that complexity. We hope that this Guide will help readers: (1)
become aware of how best to study the complex change processes inherent
in any educational program, and (2) understand how appreciating program
complexity and focusing on change-related outcomes in their evaluation
processes will strengthen their work.
Program evaluation is
an essential responsibility
for anyone overseeing
a medical education
program.
...educational programs
are fundamentally about
change.
3
Guide 67: Program evaluation models and related theories
In this Guide, we rst briey dene program evaluation, discuss reasons for
conducting educational program evaluation, and outline some theoretical
bases for evaluation models. We then focus on several commonly used program
evaluation models in the context of those theoretical bases. In doing so, we
describe each selected model, provide sample evaluation questions typically
associated with the model, and then discuss what that model can and cannot
do for those who use it. We recommend that educators rst identify the theories
they nd most relevant to their situation and, with that in mind, then choose
the evaluation model that best ts their needs. They can then establish the
evaluation questions appropriate for evaluating the educational program and
choose the data-collection processes that t their questions.
Program evaluation dened
At the most fundamental level, evaluation involves making a value judgment
about information that one has available (Cook, 2010; Durning & Hemmer,
2010). Thus educational program evaluation uses information to make a
decision about the value or worth of an educational program (Cook, 2010).
More formally dened, the process of educational program evaluation is
the “systematic collection and analysis of information related to the design,
implementation, and outcomes of a program, for the purpose of monitoring
and improving the quality and effectiveness of the program.” (ACGME, 2010a)
As is clear in this denition, program evaluation is about understanding the
program through a routine, systematic, deliberate gathering of information to
uncover and/or identify what contributes to the ‘success’ of the program and
what actions need to be taken in order to address the ndings of the evaluation
process (Durning & Hemmer, 2010). In other words, program evaluation tries
to identify the sources of variation in program outcomes both from within and
outside the program, while determining whether these sources of variation or
even the outcome itself are desirable or undesirable. The model used to dene
the evaluation process shapes that work.
Information necessary for program evaluation is typically gathered through
measurement processes. Choices of specic measurement tools, strategies,
or assessments for program evaluation processes are guided by many
factors, including the specic evaluation questions that dene the desired
understanding of the program’s success or shortcomings. In this Guide, we
dene ‘assessments’ as measurements (assessment = assay) or the strategies
chosen to gather information needed to make a judgment. In many medical
education programs data from trainee assessments are important to the
program evaluation process. There are, however, many more assessments
(measurements) that may be necessary for the evaluation process, and they
may come from a variety of sources in addition to trainee performance data.
Evaluation, as noted earlier, is about reviewing, analyzing, and judging the
importance or value of the information gathered by all these assessments.
Reasons for program evaluation
Educators often have both internal and external reasons for evaluating their
programs. Primary external reasons are often found in requirements of medical
education accreditation organizations (ACGME, 2010b; LCME, 2010), funding
sources that provide support educational innovation, and other groups or
persons to whom educators are accountable.
At the most fundamental
level, evaluation involves
making a value judgment
about information that one
has available.
4
Guide 67: Program evaluation models and related theories
A strong program evaluation process supports accountability while allowing
educators to gain useful knowledge about their program and sustain ongoing
program development (Goldie, 2006).
Evaluation models have not always supported such a range of needs. For many
years evaluation experts focused on simply measuring program outcomes
(Patton, 2011). Many time-honored evaluation models remain available for that
limited but important purpose. Newer evaluation models support learning about
the dynamic processes within the programs, allowing an additional focus on
program improvement (Stufebeam & Shinkeld, 2007; Patton, 2011). After we
describe some of the theoretical constructs that have informed both older and
newer evaluation approaches, we will describe the older quasi-experimental
evaluation model and then some of the newer, more powerful, models that are
informed by more recent theories. We have selected evaluation approaches
commonly used in medical education that illustrate the several theoretical
foundations, but there are other useful approaches that we could not include in
this limited space. The list of recommended readings at the end of this Guide will
direct interested readers to information about other evaluation approaches.
Theories that inform educational program evaluation models
We now consider theories relevant to evaluation models to set the stage for
descriptions of common or useful evaluation models. Educational evaluation
models were not developed with education theories in mind; rather, the theories
that informed thinking about science and knowledge in general underpinned
the development of evaluation models. We will therefore take somewhat of an
historical approach to describing some of those theories and their relationship to
the thinking of evaluation experts over the years. These same theories can now
inform current educators’ choices of evaluation models.
Reductionism
Many of the commonly used approaches to educational evaluation have
their roots in the Enlightenment, when understanding of the world shifted from
a model of divine intervention to one of experimentation and investigation
(Mennin, 2010c). Underlying this was an assumption of order: as knowledge
accumulated, it was expected that there would be movement from disorder
to order. Phenomena could be reduced into and understood by examining
their component parts. Because order was the norm, one would be able to
predict an outcome with some precision, and processes could be determined
(controlled or predicted) because they would ow along dened and orderly
pathways (Geyer et al., 2005). The legacy of this thinking is evident in the way
many medical education programs are organized and can even be seen in our
approaches to teaching (Mennin, 2010c).
The reductionist view, that the whole (or an outcome) can be understood
and thus predicted by investigating and understanding the contribution of
the constituent parts, is an integral part of the scientic approach that has
characterized Medicine for ve centuries. The reductionist perspective also
dominated educational evaluation throughout a major portion of its short
80-year history as a formal eld of practice (Stufebeam & Shinkeld, 2007).
This cause-effect approach to analysis requires an assumption of linearity in
A strong program
evaluation process
supports accountability
while allowing educators
to gain useful knowledge
about their program and
sustain ongoing program
development.
Educational evaluation
models were not developed
with education theories in
mind; rather, the theories
that informed thinking about
science and knowledge in
general underpinned the
development of evaluation
models.
5
Guide 67: Program evaluation models and related theories
program elements’ relationships. That is, changes in certain program elements
are expected to have a predictable impact on the outcome. A small change
would be expected to have a small impact, a large change a large impact.
The assumption of linearity is evident in some popular program evaluation
models such as the Logic Model (Frechtling, 2007) and the Before, During,
and After model (Durning et al., 2007; Durning & Hemmer, 2010). Examination
of those models shows a logical ow from beginning to end, from input to
outcome. The reductionist or linear way of thinking suggests that once the
factors contributing to an outcome are known, program success or lack of
success in achieving those outcomes can be explained. The cause-and-effect
paradigm’s impact on several of the evaluation models we describe is clear.
System theory
Although the reductionist approach brought great advances in medicine
and even medical education, concern with the approach’s limitations can
be traced back to at least Aristotle and the dictum that the ‘whole is greater
than the sum of its parts’. In other words, what we see as a nal product – an
educational program, a human being, the universe – is more than simply
a summation of the individual component parts. The appreciation that an
outcome is not explained simply by component parts but that the relationships
between and among those parts and their environment (context) are important
eventually led to formulation of a system theory. In the 20th century, this is often
attributed to Bertalanffy, a biologist who proposed a general system theory in
the 1920s (Bertalanffy, 1968; Bertalanffy, 1972). Although he recognized the roots
of his idea in earlier thinking, Bertalanffy’s approach focusing on systems was a
major step away from the reductionist tradition so dominant in scientic thinking
at the time.
Bertalanffy proposed that “the fundamental character of the living thing is its
organization, the customary investigation of the single parts and processes
cannot provide a complete explanation of the vital phenomena. This
investigation gives us no information about the coordination of parts and
processes.” (Bertalanffy, 1972) Bertalanffy viewed a system as “a set of elements
standing in interrelation among themselves and with the environment.”
(Bertalanffy, 1972) Stated another way, the system comprises the parts, the
organization of the parts, and the relationships among those parts and the
environment; these relationships are not static but dynamic and changing.
In proposing his General System Theory, Bertalanffy noted, “…...there exist
models, principles, and laws that apply to generalized systems or their
subclasses, irrespective of their particular kind, the nature of their component
elements, and the relationships or ‘forces’ between them. It seems legitimate
to ask for a theory, not of systems of a more or less special kind, but of universal
principles applying to systems in general… Its subject matter is the formulation
and derivation of those principles which are valid for ‘systems’ in general”
(Bertalanffy, 1968). Thus, in his view, an animal, a human being, and social
interactions are all systems. In the context of this Guide, an educational
program is a social system comprised of component parts, with interactions and
interrelations among the component parts, all existing within, and interacting
with, the program’s environment. To understand an educational program’s
system would require an evaluation approach consistent with system theory.
The reductionist or linear
way of thinking suggests
that once the factors
contributing to an outcome
are known, program
success or lack of success in
achieving those outcomes
can be explained.
The appreciation that an
outcome is not explained
simply by component parts
but that the relationships
between and among those
parts and their environment
(context) are important
eventually led to formulation
of a system theory.
6
Guide 67: Program evaluation models and related theories
Bertalanffy’s proposal (re)presented a way of viewing science, moving away
from reductionism, and looking for commonalities across disciplines and systems.
Thus, while his ideas about a General System Theory were initially rooted in
biology, 20th century work in mathematics, physics, and the social sciences
underscored the approach that Bertalanffy proposed: across a variety of
disciplines and science, there are common underlying principles.
“A consequence of the existence of general system properties is the
appearance of structural similarities or isomorphisms in different elds. There are
correspondences in the principles that govern the behaviour of entities that are,
intrinsically, widely different. To take a simple example, an exponential law of
growth applies to certain bacterial cells, to populations of bacteria, of animals
or humans, and to the progress of scientic research measured by the number
of publications in genetics or science in general”. (Bertalanffy, 1968)
Finally, General System Theory embraces the idea that change is an inherent
part of a system. Bertalanffy described systems as either being ‘closed’, in which
nothing either enters or leaves the system, or ‘open’, in which exchange occurs
among component parts and the environment. He believed that living systems
were open systems. Equilibrium in a system means that nothing is changing
and, in fact, could represent a system that is dying. In contrast, an open
system at steady-state is one in which the elements and interrelationships are
in balance – still active, perhaps even in opposite or opposing directions, but
active nonetheless (Bertalanffy, 1968). Furthermore, in an open system, there is
eqinality: the nal state or outcome can be reached from a variety of starting
points and in a variety of ways (much like a student becoming a physician by
going through medical school) as contrasted with a closed system in which
the outcome might be predetermined by knowing the starting point and the
conditions. We believe this view of an open system is consistent with what
occurs in an educational program: it is an open system, perhaps sometimes at
steady-state, but active.
Since the advent of General System Theory, a number of other theories have
arisen to attempt to address the principles across a variety of systems. One such
theory, Complexity theory, is growing in prominence in medical education and
thus deserves further consideration of its inuence on evaluation choices.
Complexity theory
Linear models based on reductionist theory may satisfactorily explain
phenomena that are at equilibrium, a state in which they are not changing.
Educational programs, however, are rarely in equilibrium. Medical education
programs are affected by many factors both internal and external to the
program: program participants’ characteristics, inuence of stakeholders or
regulators, the ever-changing nature of the knowledge on which a discipline
is based, professional practice patterns, and the environment in which the
educational program functions, to name only a few (Geyer et al., 2005).
Medical education programs are therefore best characterized as complex
systems, given that they are made up of diverse components with interactions
among those components. The overall system cannot be explained by
separately examining each of its individual components (Mennin, 2010b).
In a sense, the program’s whole is greater than the sum of its parts – there is
more going on in the program (the complex system) than can be explained
General System Theory
embraces the idea that
change is an inherent part of
a system.
Linear models based
on reductionist theory
may satisfactorily explain
phenomena that are at
equilibrium, a state in which
they are not changing.
Educational programs,
however, are rarely in
equilibrium.
7
Guide 67: Program evaluation models and related theories
by studying each component in isolation. This might, in fact, explain the
phenomenon in educational research in which much of the variance in the
outcome of interest is not explained by factors identied in the system or
program: there is more occurring in the program with respect to explaining the
outcome than can be fully appreciated with reductionist or linear approaches
to inquiry.
Complexity theory and complexity science are attempts to embrace the
richness and diversity of systems in which ambiguity and uncertainty are
expected. “Complexity ‘science’ then is the study of nonlinear dynamical
interactions among multiple agents in open systems that are far from
equilibrium.” (Mennin, 2010c) “Complexity concepts and principles are
well suited to the emergent, messy, nonlinear uncertainty of living systems
nested one within the other where the relationship among things is more
than the things themselves.” (Mennin, 2010a) Complexity theory allows us to
accommodate the uncertainty and ambiguity in educational programs as
we think about evaluating them. It actually promotes our understanding of
such natural ambiguity as a normal part of the systems typical of medical
educational programs. Ambiguity and uncertainty are neither good nor bad
but simply expected and anticipated. Evaluating an educational program
would therefore include exploring for those uncertainties. In fact, complexity
theory invites educators to cease relying on overly simple models to explain
or understand complex educational events. “To think complexly is to adopt a
relational, a system(s) view. That is to look at any event or entity in terms, not of
itself, but of its relations.” (Doll & Trueit, 2010)
The importance of program context is part of complexity theory, helping us
to realize the “work of the environment [in] shaping activity rather than the
cognition of practitioners dictating events.”(Doll & Trueit, 2010) In other words,
examining a program’s success must not only include references to elements
related to program participants but also to the relationships of participants
with each other and with the environment in which they act and how that
environment may affect the participants.
Complexity theory can inform our choice of program evaluation models. For
example, the concept of program elements’ relationship is prominent in the
CIPP evaluation model in which Context studies play a critical role in shaping
the approach to evaluating program effectiveness and in which program
Process studies are separate but of equal importance (Stufebeam & Shinkeld,
2007). The need to understand relationships among program elements prompts
educators to include a variety of stakeholder views when developing a program
evaluation, as each one will reect key elements of the program components’
relationships. The Before, During, After evaluation model (Durning et al., 2007,
Durning & Hemmer, 2010), described in the literature but not discussed in this
Guide, can also be interpreted from the perspective of complexity theory. While
there is a linear or orderly nature to that model, it is general and generic enough
to allow program planners to envision the rich complexities possible in each
program phase and to think broadly about what elements and relations are
important within each phase.
Complexity theory and
complexity science are
attempts to embrace the
richness and diversity of
systems in which ambiguity
and uncertainty are
expected.
Examining a program’s
success must not only
include references to
elements related to program
participants but also to the
relationships of participants
with each other and with
the environment in which
they act and how that
environment may affect the
participants.
8
Guide 67: Program evaluation models and related theories
Doll suggests that “…the striving for certainty, a feature of western intellectual
thought since the times of Plato and Aristotle, has come to an end. There is no
one right answer to a situation, no formula of best practices to follow in every
situation, no assurance that any particular act or practice will yield the results
we desire.” (Doll & Trueit, 2010) We believe that appropriately chosen evaluation
models allow academic managers and educators to structure useful program
evaluations that accommodate a program’s true complexity. Complexity
theory provides a different and useful perspective for choosing an evaluation
model that serves program needs more effectively, allowing educators to avoid
an overly narrow or simplistic approach to their work.
Common evaluation models
‘Educational evaluation’ is best understood as a family of approaches
to evaluating educational programs. The following discussion of selected
evaluation models places them in relationship to the theoretical constructs
that informed their development. Thoughtful selection of a specic evaluation
model allows educators to structure their planning and to assure that important
information is not overlooked.
We will describe four models in this Guide: the familiar experimental/quasi-
experimental approach to evaluation; Kirkpatrick’s approach; the Logic Model;
and the Context/Input/Process/Product (CIPP) model. Educators will nd other
models in the evaluation literature, but these four are currently in common use
and provide clear contrasts among the possibilities offered by models informed
by different theories. Each model will be described in some detail, including
typical evaluation questions, and what the evaluator might expect when using
the model.
The experimental/quasi-experimental models
Experimental and quasi-experimental designs were some of the earliest designs
applied as educational evaluation came into common use in the mid-1960s
(Stufebeam & Shinkeld, 2007). Arising from the reductionist theoretical
foundation, the validity of ndings from studies using these designs depends on
the evaluator’s careful validation of the assumption of linear causal relationships
between program elements and desired program outcomes. These designs
explicitly isolate individual program elements for study, consistent with the
classic reductionist approach to investigation. The familiar experimental and
quasi-experimental designs were enormously useful in advancing the biological
sciences over the last century (Stufebeam & Shinkeld, 2007). They have
proven less useful in the complex environments of educational programs: true
experimental, tightly controlled designs are typically very difcult to implement
in educational programs as complex as those in medical education. Educators
usually need to compare a new way of doing things to the old way of doing
things rather than to ‘doing nothing’, so the experimental study’s outcomes
are usually measures of a marginal increment in value. Quasi-experimental
designs are used more often than the true experimental designs that are simply
not feasible. Contemporary evaluators shying away from experimental or
quasi-experimental designs cite low external validity due to the study design
challenges and point to the highly focused nature of such a study’s ndings.
‘Educational evaluation’ is
best understood as a family
of approaches to evaluating
educational programs.
Educators usually need
to compare a new way
of doing things to the old
way of doing things rather
than to ‘doing nothing’, so
the experimental study’s
outcomes are usually
measures of a marginal
increment in value.
9
Guide 67: Program evaluation models and related theories
We now describe and comment on the most commonly used quasi-
experimental designs seen in evaluation studies, as those models persist in
medical education practice. Educators should be familiar with them in order to
make informed choices for their own work.
In the Intact-Group Design, learners are randomly assigned to membership
in one of two groups. The program being evaluated is used by one of the
two groups; the other gets the usual (unchanged) program. The use of
randomization is intended to control all factors operating within the groups’
members that might otherwise affect program outcomes. Based on the learners’
random assignment to groups, the evaluator then acts on the assumption that
each group member is an individual replication of the program state (new
program or old program). If, for example, each group had 30 members then
the analysis would be of n=60 rather than n=2 (groups). For optimal use of this
evaluation design, the intact-groups study should be repeated multiple times. If
repetition is not feasible, the evaluator/experimenter must continually be alert
for unexpected differences that develop between the groups that are not due
to the planned program implementation. For example, one group might miss
a planned program element due to an event outside the educator’s control,
such as an unplanned faculty absence. The evaluator/experimenter in this
dynamic environment must then attempt adjustments to negate the potential
inuence of that factor on one group. If the assumption of a linear relationship
between the ‘input’ (program type) and the ‘outcome’ is logically defensible
and if random assignment to groups has been achieved and maintained, the
educator must also guarantee that the programs being compared have been
implemented with delity and that the impact of unintended events has been
equalized.
Evaluators who choose a Time-Series Experimental Design study the behavior
of a single person or group over time. By observing the learner(s) or group(s)
before a new program is implemented, then implementing the program, and
nally conducting the same observations after the program, the evaluator
can compare the pre- and post-program behaviors as an assessment of the
program’s effects. This design is similar to the pre/post test design well-known to
educators. Time-series studies are most useful when the program is expected
to make immediate and long-lasting changes in behavior or knowledge.
The number of observations required both pre- and post-program for reliable
assessment of changes must be carefully considered. The design does not
separate the effects that are actually due to the program being evaluated
from effects due to factors external to the program, e.g., learner maturation,
learning from concurrent courses or programs, etc. A variation on the time-series
design uses different learner groups; for example, learners in early phases of
a longitudinal program over several years may be observed to gather pre-
program data, while other learners who used the program may be observed
to gather post-program data. This requires the evaluator to collect sufcient
data to defend the assumption that the ‘early phase’ learners are consistently
the same with respect to characteristics relevant to the program even though
the learners observed pre-program are not the same as those observed post-
program. For example, all learners in the rst year of post-graduate training
at Institution X might be observed for two years to collect data about their
advanced clinical procedural skills. At the same time, an intensive new program
designed to teach advanced clinical procedural skills might be introduced for
10
Guide 67: Program evaluation models and related theories
nal-year post-graduate trainees at that institution and data collected after the
program for the rst two groups (two years) to go through that program. Then
the evaluator would compare the early-phase learner data to the post-program
learner data, although the groups do not contain the same individuals. The
usefulness of this design is limited by the number of design elements that must
be logically defended, including assumptions of linear relationships between
program elements and desired outcomes, stability of outcome variables
observed over a short time period, or (in the case of using different learner
groups) sufcient comparability of comparison groups on outcome-related
variables.
The Ex Post Facto Experiment Design, though criticized by some evaluation
experts, may be useful in some limited contexts. In this design the evaluator
does not use random assignment of learners to groups or conditions. In fact,
the evaluator may be faced with a completed program for which some
data have been collected but for which no further data collection is feasible.
Realizing the weakness of the design, its appropriate use requires analyzing
outcome variables after every conceivable covariate has been included in
the analysis model (Lieberman et al., 2010). The evaluator must therefore have
access to relevant pre-program participant data to use as covariates. When
those covariates are even moderately correlated with program outcomes, the
program effects may not be detectable with this study design, and a nding of
‘no effect’ may be unavoidable.
What can evaluators expect to gain from experimental and quasi-experimental
models? Reductionist approaches are familiar to most medical educators, so
experimental and quasi-experimental evaluation studies offer the comfort of
familiar designs. The designs do require assumption of linear causal relationships
between educational elements and outcomes, although the complexity of
educational programs can make it difcult to document the appropriateness
of those assumptions. It can also be difcult simply to implement studies of this
type in medical education because learning institutions are not constructed
like research environments – they rarely support the randomization upon
which true experimental designs are predicated. Ethical considerations must
be honored when random assignment would keep learners from a potentially
useful or improved learning experience. In many educational situations,
even quasi-experimental designs are difcult to implement. For example,
institutional economics or other realities that cannot be manipulated may
make it impossible to conduct an educational activity in two different ways
simultaneously. When both feasible and logically appropriate to use these
designs, evaluators may choose them when high internal validity of ndings
is valued over the typically low external validity yielded by experimental and
quasi-experimental designs. These designs, used alone, can sometimes provide
information about the educational activity’s outcomes but cannot provide
evidence for why the outcomes were or were not observed.
Kirkpatrick’s four-level evaluation model
Kirkpatrick’s four-level approach has enjoyed wide-spread popularity as a
model for evaluating learner outcomes in training programs (Kirkpatrick, 1996).
Its major contributions to educational evaluation are the clarity of its focus
on program outcomes and its clear description of outcomes beyond simple
learner satisfaction. Kirkpatrick recommended gathering data to assess four
Kirkpatrick’s four-level
approach has enjoyed
wide-spread popularity
as a model for evaluating
learner outcomes in
training programs. Its major
contributions to educational
evaluation are the clarity
of its focus on program
outcomes and its clear
description of outcomes
beyond simple learner
satisfaction.
11
Guide 67: Program evaluation models and related theories
hierarchical ‘levels’ of program outcomes: (1) learner satisfaction or reaction
to the program; (2) measures of learning attributed to the program (e.g.,
knowledge gained, skills improved, attitudes changed); (3) changes in learner
behavior in the context for which they are being trained; and (4) the program’s
nal results in its larger context. To assess learner reactions to the program,
evaluators would determine the desired reactions (satisfaction, etc.) and ask
the learners what they thought about the program. Learners might be asked,
for example, if they felt the program was useful for learning and if individual
components were valuable. The second Kirkpatrick ‘level’ requires the evaluator
to assess what participants learned during the program. Various designs can
be used to attempt to connect the learning to the program and not to other
learning opportunities in the environment. Tests of knowledge and skills are
often used, preferably with an appropriate control group, to investigate this
aspect. A ‘level three’ Kirkpatrick evaluation focuses on learner behavior in the
context for which they were trained (e.g., application of knowledge previously
gained to a new standardized patient encounter). For example, post-graduate
trainees’ use of the program’s knowledge and skills might be observed in their
practice setting and compared to the desired standard to collect evidence for
a ‘level three’ evaluation. A ‘level four’ Kirkpatrick evaluation focuses on learner
outcomes observed after a suitable period of time in the program’s larger
context: the program’s impact, for example, on patient outcomes, cost savings,
improved healthcare team performance, etc.
Kirkpatrick’s model has been criticized for what it does not take into account,
namely intervening variables that affect learning (e.g., learner motivation,
variable entry levels of knowledge and skills), relationships between important
program elements and the program’s context, the effectiveness of resource
use, and other important questions (Holton, 1996). The model requires the
assumption of causality between the educational program and its outcomes, a
reection of the reductionist linear theories.
What can evaluators gain from using the Kirkpatrick four-level approach?
Kirkpatrick’s approach denes a useful taxonomy of program outcomes (Holton,
1996). By itself, however, the Kirkpatrick model is unlikely to guide educators
into a full evaluation of their educational program (Bates, 2004) or provide data
to illuminate why a program works. Used in conjunction with another model,
however, Kirkpatrick’s four levels may offer a useful way to dene the program
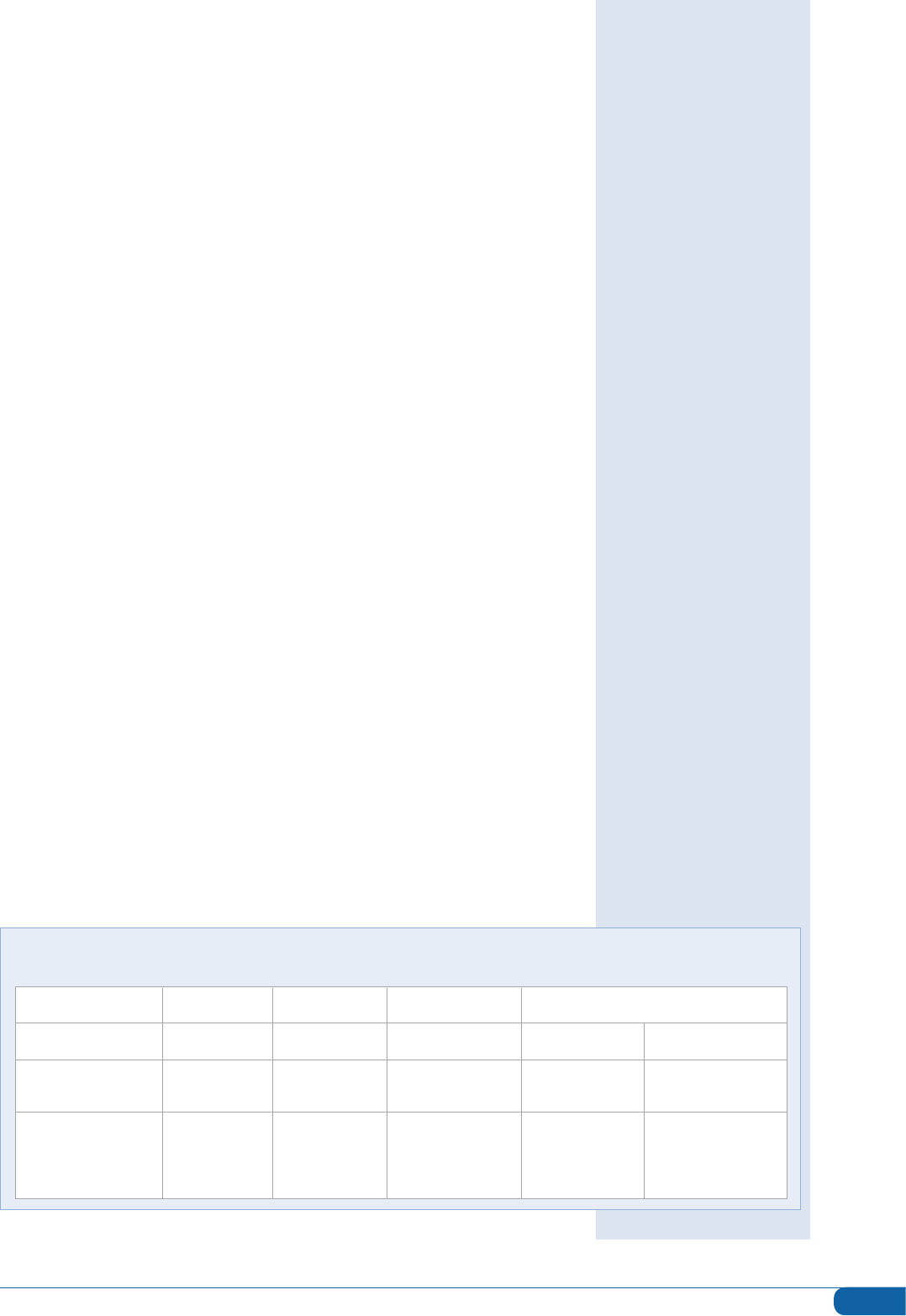
outcomes element of other more complete evaluation models (Table 1).
Kirkpatrick’s model has been
criticized for what it does not
take into account, namely
intervening variables that
affect learning.
TABLE 1:
Comparison of Evaluation Models
CIPP Studies Context Studies Input Studies Process Studies Product Studies
Logic Model Input element → Activities element → Output element→ Outcomes element
Kirkpatrick’s Learner-related
4-level model outcomes
Experimental quasi- Linear relationship
experimental models of intended program
outcomes to
program elements
12
Guide 67: Program evaluation models and related theories
The Logic Model
The inuence of system theory on the Logic Model approach to evaluation
can be seen in its careful attention to the relationships between program
components and the components’ relationships to the program’s context.
(Frechtling, 2007) Though often used during program planning instead of
solely as an evaluation approach, the Logic Model structure strongly supports
a rational evaluation plan. The Logic Model, similar to the evaluation models
already discussed, can be strongly linear in its approach to educational
planning and evaluation. In its least complicated form, it may oversimplify the
program evaluation process and thus not yield what educators need. With
careful attention to building in feedback loops and to the possibility of circular
interactions between program elements, however, the Logic Model can offer
educators an evaluation structure that incorporates system theory applications
into thinking about educational programs. The Logic Model approach to
program evaluation is currently promoted or required by some U.S. funding
agencies (Frechtling, 2007), so it is worth knowing what this approach can offer.
The Logic Model’s structure shares characteristics with Stufebeam’s CIPP
evaluation model (Table 1) but focuses on the change process and the system
within which the educational innovation is embedded. Though its structural
simplicity makes it attractive to both novice and experienced educators,
this approach is grounded in the assumption that the relationships between
the program’s educational methods and the desired outcomes are clearly
understood. The simplest form of the Logic Model approach may therefore
oversimplify the nonlinear complexity of most educational contexts. The
Logic Model works best when educators clearly understand their program
as a dynamic system and plan to document both intended and unintended
outcomes.
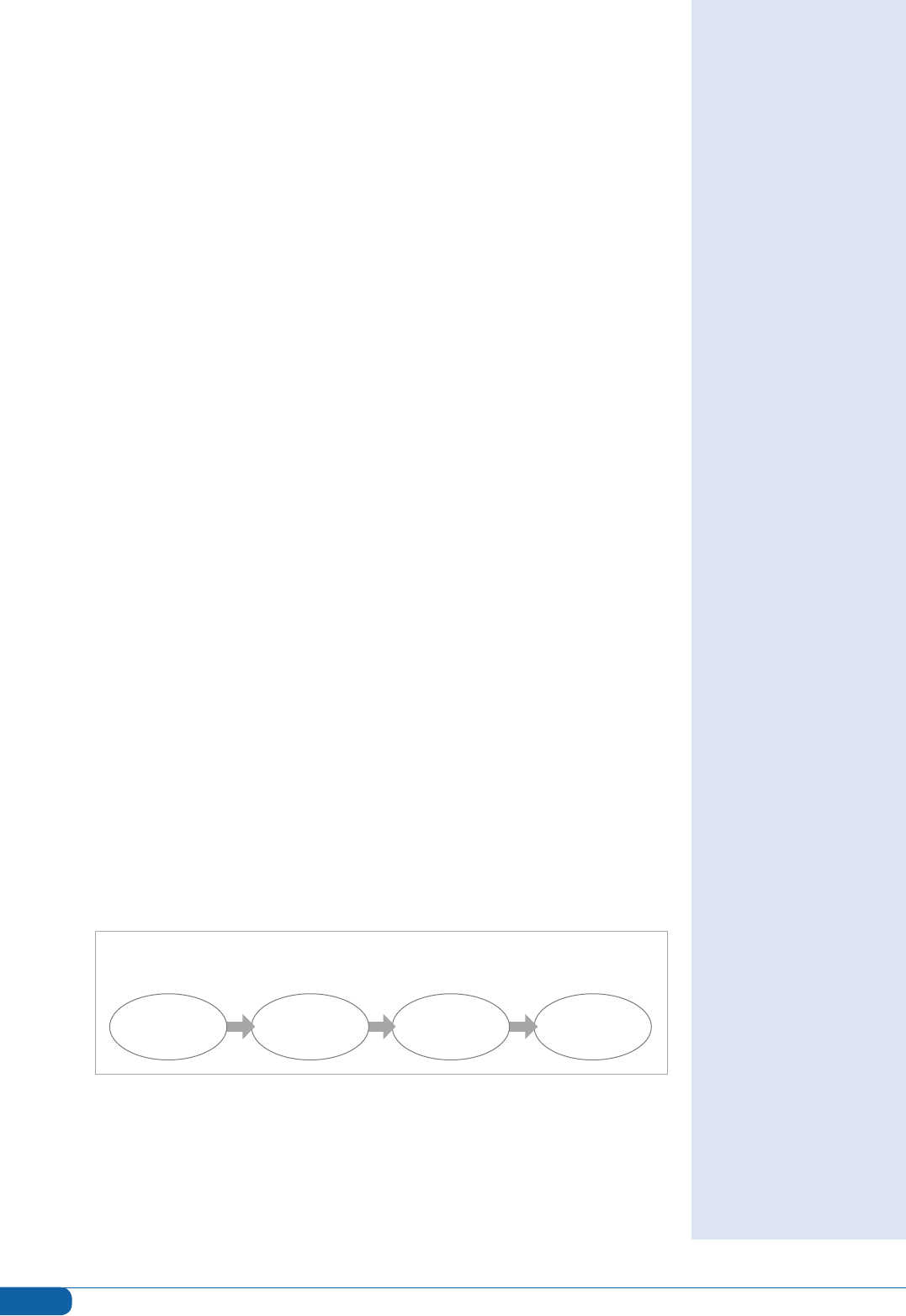
The four basic components of the Logic Model are simple to dene (Figure 1).
The level of complexity introduced into the specication of each component
can vary with the evaluator’s skill or the program director’s resources. When
using a Logic Model for program planning, most nd it useful to begin with the
desired Outcomes and then work backwards through the other components
(Frechtling, 2007). For complex programs, the Logic Model can be expanded
to multiple tiers. Our description will include only the basics of the four essential
elements, but details of multi-tiered Logic Models suitable for more complex
programs are readily available in texts (Frechtling, 2007).
FIGURE 1:
Logic Model Components
The inuence of system
theory on the Logic Model
approach to evaluation
can be seen in its careful
attention to the relationships
between program
components and the
components’ relationships to
the program’s context.
The Logic Model works best
when educators clearly
understand their program as
a dynamic system and plan
to document both intended
and unintended outcomes.
INPUTS ACTIVITIES OUTPUTS OUTCOMES
13
Guide 67: Program evaluation models and related theories
• INPUTS: A Logic Model’s Inputs comprise all relevant resources, both material
and intellectual, expected to be or actually available to an educational
project or program. Inputs may include funding sources (already on hand
or to be acquired), facilities, faculty skills, faculty time, staff time, staff skills,
educational technology, and relevant elements of institutional culture (e.g.,
Departmental or Dean’s support). Dening a program’s Inputs denes a
new program’s starting point or the current status of an existing program.
Importantly, an inventory of relevant resources allows all stakeholders an
opportunity to conrm the commitment of those resources to the program. A
comprehensive record of program resources is also useful later for describing
the program to others who may wish to emulate it. Readers of this Guide may
nd it helpful to cross-reference the Input section of the Logic Model to the
Input section of Stufebeam’s CIPP model (Table 1). The CIPP model’s Input
section is a more detailed way of looking at program ‘inputs’ and can be
used to expand the construction of the Logic Model’s input section.
• ACTIVITIES: The second component of a Logic Model details the Activities,
the set of ‘treatments’, strategies, innovations or changes planned for the
educational program. Activities are typically expected to occur in the order
specied in the Model. That explicit ordering of activities acknowledges that
a subsequent activity may be inuenced by what happens after or during
implementation of a preceding activity. Educators working with complex
multi-activity programs are urged to consult a reliable text on the Logic
Model for suggestions about developing more elaborated models to meet
the needs of their programs (e.g., Frechtling, 2007).
• OUTPUTS: Outputs, the Logic Model’s third component, are dened as
indicators that one of the program’s activities or parts of an activity is
underway or completed and that something (a ‘product’) happened.
The Logic Model structure dictates that each Activity must have at least
one Output, though a single Output may be linked to more than one
Activity. Outputs can vary in ‘size’ or importance and may sometimes be
difcult to distinguish from Outcomes, the fourth Logic Model component.
In educational programs, Outputs might include the number of learners
attending a planned educational event (the activity), the characteristics of
faculty recruited to contribute to the program (if, for example, ‘recruit faculty
with appropriate expertise’ were a program activity), or the number of
educational modules created or tested (if, for example, ‘create educational
modules’ were an activity).
• OUTCOMES: Outcomes dene the short-term, medium-term, and longer-
range changes intended as a result of the program’s activities. A program’s
Outcomes may include learners’ demonstration of knowledge or skill
acquisition (e.g., meeting a performance standard on a relevant knowledge
test or demonstrating specied skills), program participants’ implementation
of new knowledge or skills in practice, or changes in health status of program
participants’ patients. Outcomes may be specied at the level of individuals,
groups or an organization (e.g., changes in a department’s infrastructure to
support education). Cross-referencing to Stufebeam’s CIPP model’s Product
section may provide additional ideas for the Outcomes section of a Logic
Model (Table 1).
14
Guide 67: Program evaluation models and related theories
In addition to the four basic Logic Model elements, a complete Logic Model
is carefully referenced to the program’s Context and its Impacts. Context
refers to important elements of the environment in which the program takes
place, including social, cultural, and political features. For example, when
a governmental or accrediting body mandates a new topic’s inclusion in
a curriculum, this is a relevant political factor. Learner characteristics may
be relevant social factors. Attending to contextual features of a program’s
environment that may limit or support the program’s adoption by others helps
planners to identify program elements that should be documented. Impact
comprises both intended and unintended changes that occur after a program
or intervention. Long-term outcomes with a very wide reach (e.g., improving
health outcomes for a specic group) might be better dened as ‘impacts’
than outcomes in a Logic Model approach.
The Logic Model approach can support the design of an effective evaluation
if educators are appropriately cautious of its linear relationship assumptions.
Typical evaluation questions that might be used in a Logic Model approach
include questions like these:
• Was each program activity implemented as planned? If changes from the
planned activities were made, what changes were made and why were
they necessary?
• Were the anticipated personnel available? Did they participate as
anticipated? Did they have the required skills and experience?
• How well did the activities meet the needs of all learners, including learner
groups about which the program might be especially concerned?
• What barriers to program implementation were encountered? How was the
planned program modied to accommodate them?
• Did faculty participate in associated faculty development? What skills or
knowledge did they acquire? How well did they implement what they
learned in program activities?
• How did participants in the program activities evaluate the activities for
effectiveness, accessibility, etc.?
• What were learners’ achievement outcomes?
• How often or how well did learners apply what they learned in their clinical
practice?
• How did related patient outcomes change after program implementation?
What should educators expect to gain from using the Logic Model approach? A
Logic Model approach can be very useful during the planning phases of a new
educational project or innovation or when a program is being revised. Because
it requires that educational planners explicitly dene the intended links between
the program resources (Inputs), program strategies or treatments (Activities),
the immediate results of program activities (Outputs), and the desired program
accomplishments (Outcomes), using the Logic Model can assure that the
educational program, once implemented, actually focuses on the intended
outcomes. It takes into account the elements surrounding the planned change
(the program’s context), how those elements are related to each other, and
how the program’s social, cultural, and political context is related to the
planned educational program or innovation.
Logic Model approach
can be very useful during
the planning phases of a
new educational project
or innovation or when a
program is being revised.
15
Guide 67: Program evaluation models and related theories
Logic Models have proven especially useful when more than one person is
involved in planning, executing, and evaluating a program. When all team
members contribute to the program’s Logic Model design, the conversations
necessary to reach shared understandings of program activities and desired
outcomes are more likely to happen. Team members’ varied areas of expertise
and their different perspectives on the theory of change pertinent to the
program’s activities and desired outcomes can inform the program’s design
during this process.
Some potential pitfalls of using the Logic Model should be considered, however.
Its inherent linearity (Patton, 2011) can focus evaluators on blindly following
the Model during program implementation without looking for unanticipated
outcomes or exibly accommodating mid-stream program changes. Evaluators
aware of this pitfall will augment the Logic Model approach with additional
strategies designed to capture ALL program outcomes and will adapt the
program’s activities (and the program’s Logic Model) as needed during
program implementation. A program’s initial Logic Model may need to be
revised as the program is implemented.
The Logic Model approach works best when the program director or team
has a well-developed understanding of how change works in the educational
program being evaluated. A program’s Logic Model is built on the stakeholders’
shared understandings of which strategies are most likely to result in desired
outcomes (changes) and why, so users should draw on research and their own
experience as educators to hypothesize how change will work in the program
being evaluated. In all cases, however, evaluators should be aware of and
explore alternative theories of change that may be operating in the program.
The Logic Model approach will not generate evidence for causal linkages
of program activities to outcomes. It will not allow the testing of competing
hypotheses for the causes of observed outcomes. If carefully implemented, it
can, however, generate ample descriptive data about the program and the
subsequent outcomes.
The CIPP (Context/Input/Process/Product) model
The CIPP set of approaches to evaluation is described by Daniel Stufebeam,
its creator, as his response to and improvement on the dominant experimental
design model of its time (Stufebeam & Shinkeld, 2007). First described in print
in 1971, Stufebeam intended CIPP Model evaluations to focus on program
improvement instead of proving something about the program. The usefulness
of the CIPP model across a variety of educational and non-educational
evaluation settings has been thoroughly documented (Stufebeam and
Shinkeld, 2007). Its elements share labels with the Logic Model (Table 1), but
the CIPP model is not hampered by the assumption of linear relationships that
constrains the Logic Model. An evaluator who understands an educational
program in terms of its elements’ complex, dynamic and often nonlinear
relationships will nd the CIPP model a powerful approach to evaluation.
The CIPP approach consists of four complementary sets of evaluation studies
that allow evaluators to consider important but easily overlooked program
dimensions. Taken together, CIPP components accommodate the ever-
changing nature of most educational programs as well as educators’ appetite
The Logic Model approach
will not generate evidence
for causal linkages of
program activities to
outcomes. It will not allow
the testing of competing
hypotheses for the causes of
observed outcomes.
Stufebeam intended CIPP
Model evaluations to focus
on program improvement
instead of proving something
about the program.

16
Guide 67: Program evaluation models and related theories
for program-improvement data. By alternately focusing on program Context,
Inputs, Process, and Products, the CIPP model addresses all phases of an
education program: planning, implementation, and a summative or nal
retrospective assessment if desired. The rst three elements of the CIPP model
are useful for improvement-focused (formative) evaluation studies, while the
Product approach, the fourth element, is very appropriate for summative (nal)
studies.
• Context evaluation study: A CIPP Context evaluation study is typically
conducted when a new program is being planned. The associated
evaluation questions (Table 2) are also useful when an established program
is undergoing planned change or must adapt to changed circumstances. A
new leader taking over an existing program, for example, may nd thinking
through a Context evaluation study helpful. Context studies can also be
conducted when decisions about cutting existing programs are necessary.
Explicit attention to an educational program’s context is essential to effective
evaluation and aligns well with complexity theory’s emphasis on context.
TABLE 2:
Evaluation questions common to CIPP evaluation studies
CONTEXT
• What is necessary or useful:
in other words, what are the
educational needs?
• What are the impediments
to meeting necessary or
useful needs?
• What pertinent expertise,
services, or other assets are
available?
• What relevant opportunities
(e.g., funding opportunities,
administrative support)
exist?
INPUT
• What are the potential
approaches to meeting
the identied educational
need?
• How feasible is each of
the identied approaches,
given the specic
educational context of
the need?
• How cost-effective is each
identied approach,
given the specic
educational context of
the need?
PROCESS
• How was the program
actually implemented,
compared to the plan?
• How is/was the program
implementation
documented?
• Are/were program activities
on schedule? If not, why?
• Is/was the program running
on budget? If it is/was over or
under the planned budget,
why?
• Is/was the program running
efciently? If not, why?
• Can/did participants accept
and carry out their roles?
• What implementation
problems have been/were
encountered?
• How well are/were the
implementation problems
addressed?
• What do/did participants
and observers think about the
quality of the process?
PRODUCT
• What positive outcomes
of the program can be
identied?
• What negative outcomes
of the program can be
identied?
• Were the intended outcomes
of the program realized?
• Were there unintended
outcomes, either positive or
negative?
• What are the short-term
implications of program
outcomes?
• What are the longer-term
implications of program
outcomes?
• What impacts of the program
are observed?
• How effective was the
program?
• How sustainable is the
program?
• How sustainable are the
intended and positive
program outcomes?
• How easily can the program
elements be adopted by
other educators with similar
needs?
17
Guide 67: Program evaluation models and related theories
A CIPP Context evaluation study identies and denes program goals and
priorities by assessing needs, problems, assets, and opportunities relevant
to the program. The Context study’s ndings provide a useful baseline
for evaluating later outcomes (Products). When preparing a request for
external funding, a program’s planning or leadership team can use a good
Context study to strengthen the proposal. Because questions about potential
impediments and assets are included, a Context evaluation is more inclusive
than a conventional ‘needs assessment’, though it does include that essential
element.
A number of data collection and analysis methods lend themselves well
to a Context study. The evaluator might select from among the following
methods, for example, depending on what the situation demands:
– Document review
– Demographic data analysis
– Interviews
– Surveys
– Records analysis (e.g., test results, learner performance data)
– Focus groups
• Input evaluation study: A CIPP model Input evaluation study is useful
when resource allocation (e.g., staff, budget, time) is part of planning
an educational program or writing an educational proposal. An Input
evaluation study assesses the feasibility or cost-effectiveness of alternative or
competing approaches to the educational need, including various stafng
plans and ways to allocate other relevant resources. Incorporating the Input
evaluation approach into program development helps to maintain maximum
responsiveness to unfolding program needs (context). Building on the
associated Context evaluation study, a CIPP model Input evaluation study
focuses on how best to bring about the needed changes. A well-conducted
Input evaluation study prepares educators to explain clearly why and how a
given approach was selected and what alternatives were considered.
A CIPP Input evaluation study formalizes a scholarly approach to program
design. When used to plan a new program, an Input evaluation study can
also set up clear justication for assigning grant funding or other critical
resources to a new program. When applied to a program already in
place, an Input evaluation study can help the educator to assess current
educational practices against other potential practices. Its focus on feasibility
and effectiveness allows a developing program to remain sensitive to the
practices most likely to work well.
Identifying and assessing potential approaches to an educational need in an
Input study might involve any of the following methods:
– Literature review
– Visiting exemplary programs
– Consulting experts
– Inviting proposals from persons interested in addressing the identified
needs
18
Guide 67: Program evaluation models and related theories
• Process evaluation study: A CIPP Process evaluation study is typically used
to assess a program’s implementation. This type of study also prepares
the evaluator to interpret the program’s outcomes (see Product study) by
focusing attention on the program elements associated with those outcomes.
A Process evaluation study can be conducted one or more times as a
program runs to provide formative information for guiding in-process revisions.
For programs operating in the complex environment typical of medical
education programs, this attention to process issues allows an ongoing data
ow useful for program management and ongoing effective change. This
kind of evaluation study can also be conducted after a program concludes
to help the educator understand how the program actually worked. A CIPP
Process study explicitly recognizes that an educational model or program
adopted from one site can rarely be implemented with delity in a new site:
contextual differences usually dictate minor to major adaptations to assure
effectiveness. The Process evaluation study elicits information about the
program as actually implemented. Retrospective Process evaluation studies
can also be used to examine often-overlooked but very important program
aspects.
The CIPP model’s Process evaluation study is invaluable for supporting
accountability to program stakeholders. It also allows for the data collection
necessary for a program’s continual improvement. The ‘lessons learned’
about programmatic processes documented in a Process study are often
useful to other educators, even when communication of program outcomes
alone may not be all that useful.
An evaluator designing a CIPP Process evaluation study would typically want
to use the least-obtrusive methods possible while the program is running. The
evaluator might choose from among these methods:
– Observation
– Document review
– Participant interviews
• Product evaluation study: The CIPP model’s Product evaluation study
will seem familiar to most educators because of its focus on program
outcomes. What may be more surprising is the breadth of that focus (Table
2). The CIPP Product evaluation study is the one most closely aligned to the
traditional ‘summative’ program evaluation found in other models, but it
is more expansive. This type of evaluation study aims to identify and assess
the program outcomes, including both positive and negative outcomes,
intended and unintended outcomes, short-term and long-term outcomes. It
also assesses, where relevant, the impact, the effectiveness, the sustainability
of the program and/or its outcomes, and the transportability of the program.
A CIPP model Product evaluation study also examines the degree to which
the targeted educational needs were met. A Product evaluation study may
be conducted while a project is running, as interim reports of such a study
will be useful for accountability purposes and for considering alternative
processes, if warranted by less than desirable ndings.
19
Guide 67: Program evaluation models and related theories
A well-conducted CIPP model Product evaluation study allows the evaluator
to examine the program’s outcomes across all participants as well as within
relevant sub-groups or even for individual participants. Program outcomes
(Products) are best interpreted with the ndings of the Process evaluation
studies in hand: it is possible, for example, that poor implementation
(a process issue) might cause poor or unintended outcomes. The art
of the Product evaluation study is in designing a systematic search for
unanticipated outcomes, positive or negative. To encompass the breadth
of a good Product evaluation study, the evaluator might choose from these
methods and data sources:
– Stakeholders’ judgments of the project or program
– Comparative studies of outcomes with those of similar projects or programs
– Assessment of achievement of program objectives
– Group interviews about the full range of program outcomes
– Case studies of selected participants’ experiences
– Surveys
– Participant reports of project effects
What should educators expect if they choose to use the CIPP model? CIPP
model studies can be used both formatively (during program’s processes) and
summatively (retrospectively). Careful attention to the educational context of
program is supported, including what comes before, after, or concurrently for
learners and others involved in the program, how ‘mature’ the program is (rst
run versus a program of long standing, etc.), and the program’s dependence
or independence on other educational elements. The CIPP model incorporates
attention to multiple ‘inputs’: learners’ characteristics, variability, and
preparation for learning; faculty’s preparation in terms of content expertise and
relevant teaching skills, the number of faculty available at the right time for the
program; learning opportunities, including patient census and characteristics
and other resources; adequacy of funding to support program needs and
leadership support. The CIPP model allows educators to consider the processes
involved in the program or to understand why the program’s products or
outcomes are what they are. It incorporates the necessary focus on program
products or outcomes, informed by what was learned in the preceding studies
of the program, but focuses on improvement rather than proving something
about the program. It can provide multiple stakeholders information about
the program’s improvement areas, interpretation of program outcomes, and
continuous information for accountability.
When choosing the CIPP model, educators should be aware that using
it effectively requires careful planning. It is most useful if taken up during
the planning phases of a new program but may be usefully adopted for
retrospective evaluation of a completed program. Multiple data collection
methods are usually required to do a good job with CIPP studies, and each
data set must be analyzed with methods appropriate to the data and to the
evaluation questions being addressed.
A well-conducted CIPP
model Product evaluation
study allows the evaluator
to examine the program’s
outcomes across all
participants as well as within
relevant sub-groups or even
for individual participants.
CIPP model studies can
be used both formatively
(during program’s
processes) and summatively
(retrospectively).
20
Guide 67: Program evaluation models and related theories
Conclusion
Educational programs are inherently about change: changing learners’
knowledge, skills, or attitudes; changing educational structures; developing
educational leaders; and so forth. The educators who design and implement
those programs know better than most just how complex the programs are,
and such complexity poses a considerable challenge to effective program
evaluation. Academic managers can gain insight into what different
evaluation models can do for them by considering the theories that inuenced
the development of popular evaluation models. The reductionist theory’s
strict linearity, reected in the familiar experimental and quasi-experimental
evaluation models, may be too limiting to accommodate the known complexity
of educational programs. Kirkpatrick’s four-level model of learner outcomes also
draws on the assumption of linear relationships between program components
and outcomes but may be useful in helping evaluators to identify relevant
learner outcomes. The Logic Model, often informative during program planning,
species the intended relationships between its evaluation components and
may require constant updating as a program evolves. The Logic Model’s
grounding in system theory prompts adopters to incorporate the program’s
context in evaluation studies, making it more inclusive than earlier evaluation
models. Stufebeam’s CIPP model is consistent with system theory and, to some
degree, with complexity theory: it is exible enough to incorporate the studies
that support ongoing program improvement as well as summative studies of a
completed program’s outcomes. Medical educators can choose from these
individual models or a combination of them (Table 1) to develop an evaluation
model adequate for their programs.
Declaration of interest
The authors report no declarations of interest.
Disclaimer
The views in this Guide are those of the authors and do not necessarily represent
the views of the United States Government, the United States Air Force, or other
federal agencies.
Educational programs
are inherently about
change: changing
learners’ knowledge, skills,
or attitudes; changing
educational structures;
developing educational
leaders; and so forth. The
educators who design and
implement those programs
know better than most just
how complex the programs
are, and such complexity
poses a considerable
challenge to effective
program evaluation.
21
Guide 67: Program evaluation models and related theories
References
ACGME (2010a). Accreditation Council for Graduate Medical Education: Glossary of Terms
[Online]. Accreditation Council for Graduate Medical Education. Available:
http://www.acgme.org/acWebsite/about/ab_ACGMEglossary.pdf.
ACGME (2010b). Program Director Guide to the Common Program Requirements [Online].
Accreditation Council for Graduate Medical Education. Available: http://www.acgme.
org/acWebsite/navPages/nav_commonpr.asp [Accessed January 31 2011].
BATES R (2004). A critical analysis of evaluation practice: the Kirkpatrick model and the
principle of benecence. Evaluation and Program Planning, 27: 341-347.
BERTALANFFY L (1968). General System Theory: Foundations, Development, Application.
New York, George Brazilier, Inc.
BERTALANFFY L (1972). The History and Status of General Systems Theory. The Academy of
Management Journal, 15: 407-426.
COOK DA (2010). Twelve tips for evaluating educational programs. Med Teach, 32: 296-301.
DOLL WE, JR & TRUEIT D (2010). Complexity and the health care professions. J Eval Clin
Pract, 16: 841-8.
DURNING SJ, HEMMER P & PANGARO LN (2007). The structure of program evaluation: an
approach for evaluating a course, clerkship, or components of a residency or fellowship
training program. Teach Learn Med, 19: 308-18.
DURNING SJ & HEMMER PA (2010). Program Evaluation. In: ENDE, J. (ed.) ACP Teaching
Internal Medicine. Philadelphia: American College of Physicians.
FRECHTLING J (2007). Logic Modeling Methods in Program Evaluation. San Francisco, John
Wiley & Sons.
GEYER R, MACKINTOSH A & LEHMANN K (2005). What is complexity theory? Integrating
UK and European social policy: the complexity of Europeanisation. Abington: Radcliffe
Publishing Ltd.
GOLDIE J (2006). AMEE Education Guide no. 29: evaluating educational programmes.
Med Teach, 28: 210-24.
HAWKINS RE & HOLMBOE ES (2008). Constructing an Evaluation System for an Educational
Program. In: HAWKINS RE & HOLMBOE ES (eds.) Practical Guide to the Evaluation of Clinical
Competence. Philadelphia: Mosby, Inc.
HOLTON E (1996). The awed four-level evaluation model. Human Resource Development
Quarterly, 7: 5-21.
KIRKPATRICK D (1996). Revisiting Kirkpatrick’s four-level model. Training & Development, 1:
54-59.
LCME (2010). Functions and Structure of a Medical School. Standards for Accreditation
of Medical Education Programs Leading to the M.D. Degree [Online]. Washington, D.C.:
Liaison Committee on Medical Education. Available: http://www.lcme.org/standard.htm
[Accessed January 31 2010].
LIEBERMAN S, AINSWORTH M, ASIMAKIS G, THOMAS L, CAIN L, MANCUSO M, RABEK J, ZHANG
N & FRYE A (2010). Effects of comprehensive educational reforms on academic success in a
diverse student body. Med Educ, 44: 1232-1240.
MENNIN S (2010a). Complexity and health professions education. J Eval Clin Pract, 16: 835-7.
MENNIN S (2010b). Complexity and health professions education: a basic glossary. J Eval
Clin Pract, 16: 838-40.
MENNIN S (2010c). Teaching, Learning, Complexity and Health Professions Education.
Journal of International Association of Medical Science Educators, 20: 162-165.
MUSICK DW (2006). A conceptual model for program evaluation in graduate medical
education. Acad Med, 81: 759-65.
PATTON M (2011). Developmental Evaluation: Applying Complexity Concepts to Enhance
Innovation and Use. New York, The Guilford Press.
STUFFLEBEAM D & SHINKFIELD A (2007). Evaluation Theory, Models, & Applications. San
Francisco, Jossey Bass/John Wiley & Sons, Inc.
WOODWARD CA (2002). Program Evaluation. In: NORMAN GR, VAN DER VLEUTEN CP
& NEWBLE DI (eds.) International Handbook of Research in Medical Education. Kluwer
Academic Publishers
22
Guide 67: Program evaluation models and related theories
Recommended readings
In addition to those listed in the References, the following resources are
recommended for learning more about theory and other evaluation models:
ABMA TA (2005). Responsive evaluation: Its meaning and special contribution to health
promotion. Evaluation and Program Planning, 28: 279-289.
GUBA E & LINCOLN YS (1989). Fourth generation evaluation. Beverly Hills: Sage Publications.
DONALDSON SI (2007). Program theory-driven evaluation science: Strategies and
applications. Mahwah, NJ: Erlbaum. 2007.
SHADISH WR, COOK TD & LEVITON LC (1991). Foundations of program evaluation: theories of
practice. Newbury Park, CA: Sage.
If you would like more information about AMEE and its activities, please contact the AMEE Ofce:
Association for Medical Education in Europe (AMEE), 12 Airlie Place, Dundee DD1 4HJ, UK
Tel: +44 (0)1382 381953; Fax: +44 (0)1382 381987; Email: [email protected]
www.amee.org
Scottish Charity No. SC 031618
Your invitation to join AMEE
Perhaps now more than at any other time, the scholarship of medical education and the
importance of the skills required of a teacher or trainer are being recognised. You are invited
to join AMEE, a worldwide organisation with members in over 90 countries around the world,
and become part of an international network of teachers, trainers, educators, and students
committed to encouraging excellence in teaching and learning in the health professions.
The benets of individual membership include:
• Membership of a network of individuals and institutions with
an interest in education in the health professions
• 12 monthly issues of Medical Teacher, an international
journal designed for the practicing teacher
• Access to MedEdWorld, including live webinars, a global online
medical education community (see www.mededworld.org)
• Reduced AMEE conference registration fee
• Reduced ESME Online course fee with the opportunity to
obtain an AMEE-ESME Certicate in Medical Education
• Opportunity to apply for members-only research grants and other awards
• Discount on AMEE and BEME guides
• Your achievements recognised as a member of a leading professional body
• Opportunity to participate in the wide range of AMEE activities
• One vote in the General Assembly

ISBN: 978-1-908438-18-8
For information about other guides in the series and how to order copies, please see the AMEE website:
www.amee.org
AMEE
12 Airlie Place
Dundee
DD1 4HJ
Scotland
UK
email: [email protected]
www.amee.org
Scottish Charity No. SC 031618
